Case
What is the diagnosis in 2 words?
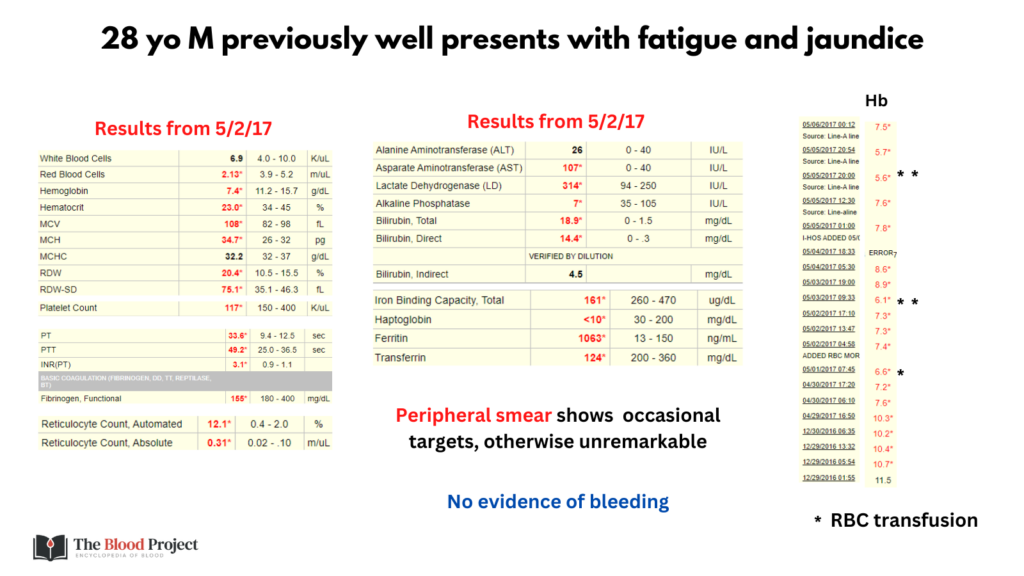
One of 13 slides

Two of 13 slides
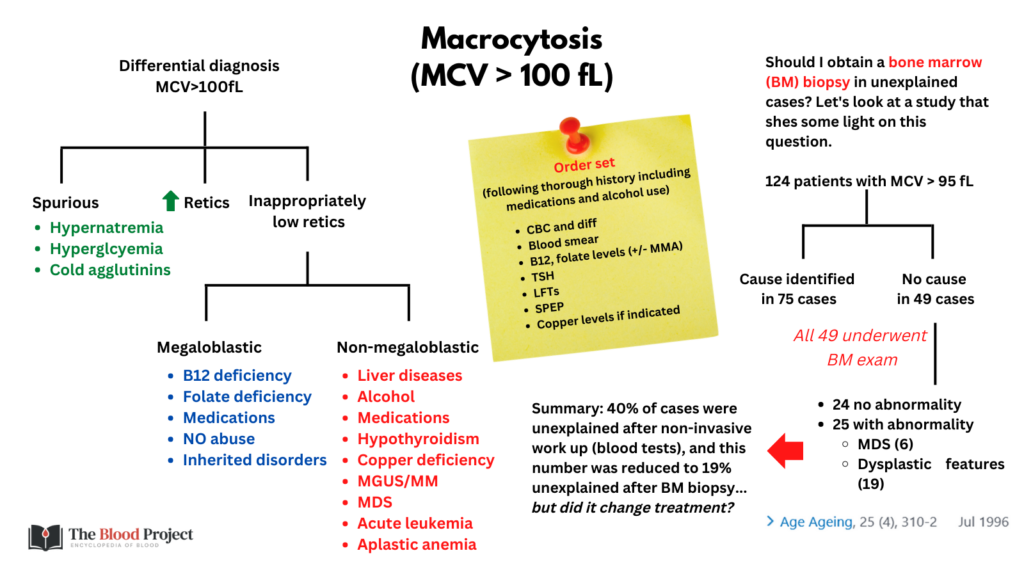
Below is a differential diagnosis for macrocytosis:
Four of 13 slides
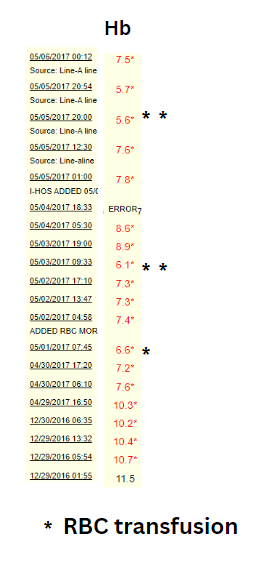
Now let’s look at the patient’s CBC over time:
Five of 13 slides
The following were the patient’s reticulocyte counts:

Six of 13 slides
On the first slide it was indicated that the patient had no evidence of bleeding. That leaves hemolysis as the most likely cause.
Seven of 13 slides
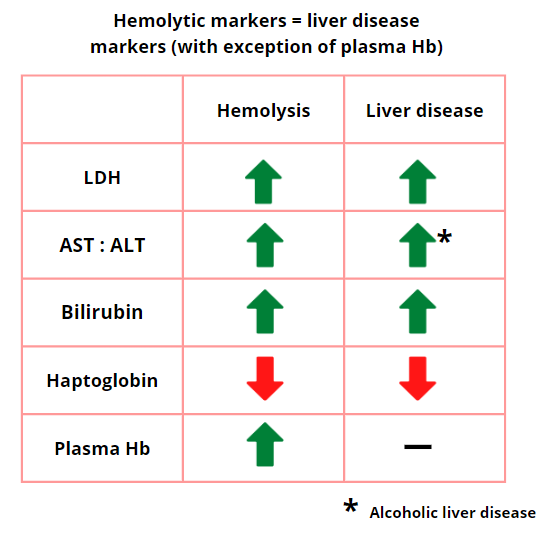
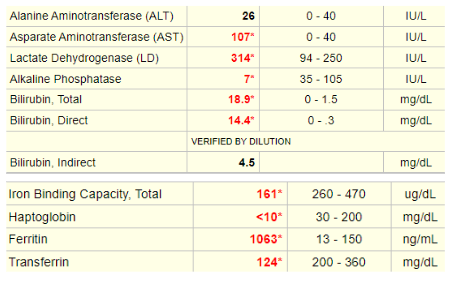
The following is a review of commonly ordered hemolytic markers. Note how closely they overlap with changes in liver disease:
Eight of 13 slides
The hemolytic markers in this patient are shown here:
These data are consistent with (more than one answer may apply):
Ten of 13 slides
Below is a differential diagnosis for hemolysis:
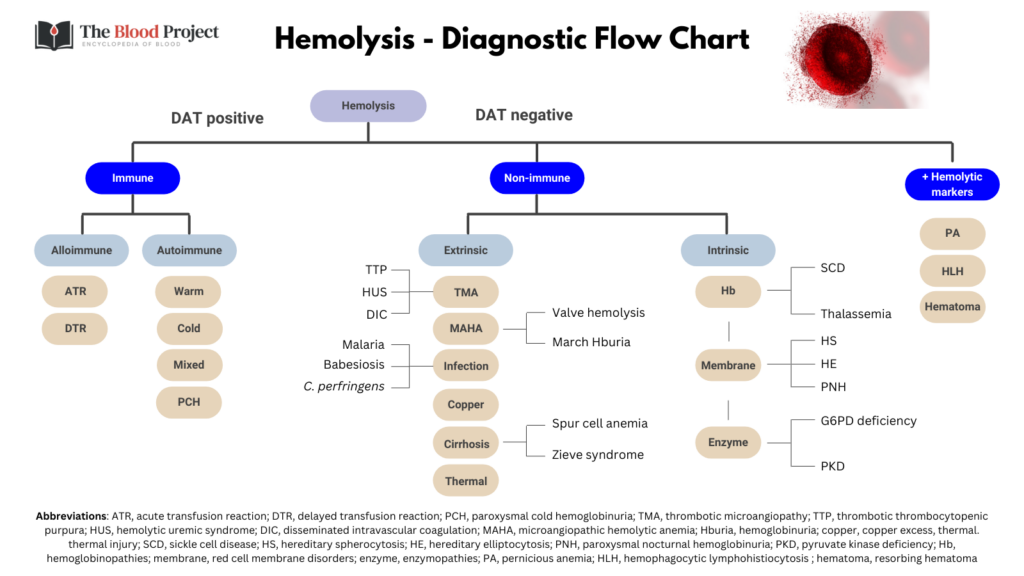
Eleven of 13 slides
So far, we have a 28 yo M, previously well, presenting with fatigue and jaundice, found to have a hyperproliferative macrocytic anemia, shorted RBC survival consistent with hemolysis, hemolytic markers consistent with both hemolysis and liver disease, and a normal blood smear. Of the diagnoses most consistent with hemolysis + normal peripheral smear (see last slide), only Wilson disease and Zieve syndrome are associated with significant liver disease. It was stated in the initial presentation that that the patient was previously well, which makes Zieve syndrome less likely (as does the extent of liver failure). Indeed, the patient was diagnosed with Wilson disease!
Note that we have approached this case from a hematological angle (for teaching purposes). Of course, when the patient was admitted, he was assessed by the liver service (and hematology, among other services, was consulted). The liver team would have used a diagnostic scoring system (e.g., the Leipzig score) to secure the diagnosis. The Leipzig score includes the following parameter:

Patient results:
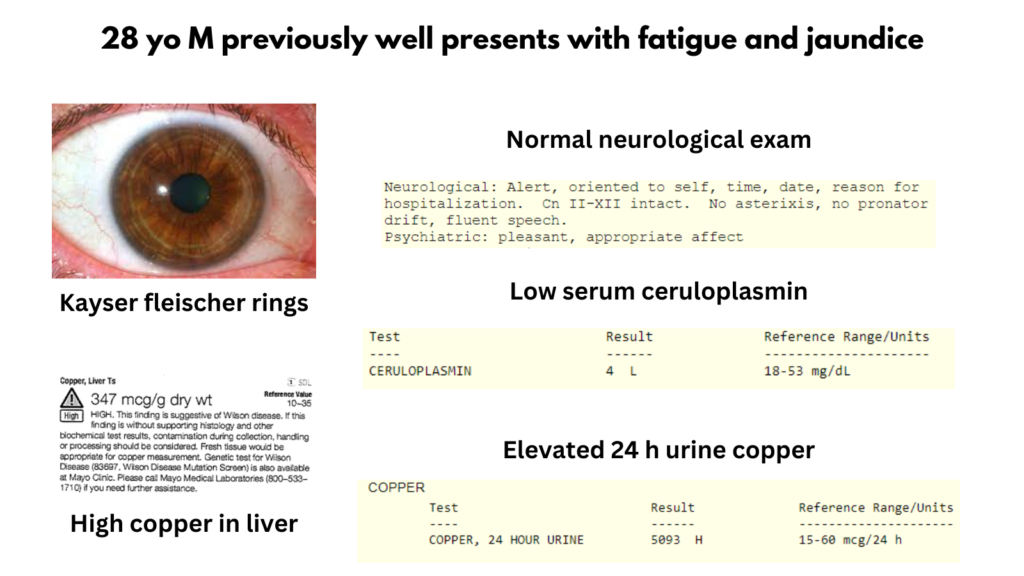
| Parameter | Value | Score |
|---|---|---|
| KF rings | Present | 2 |
| Neurological | Normal | 0 |
| Serum ceruloplasmin | 4 mg/dL | 2 |
| Coombs negative HA | Present | 1 |
| Liver copper | 347 mcg/g | 2 |
| Urinary copper | 5093 mcg | 2 |
| Mutation analysis | Not done | 0 |
| Total | 9 |
Easily meets the criteria for diagnosis of Wilson disease.
Thirteen of 13 slides