Name that CBC
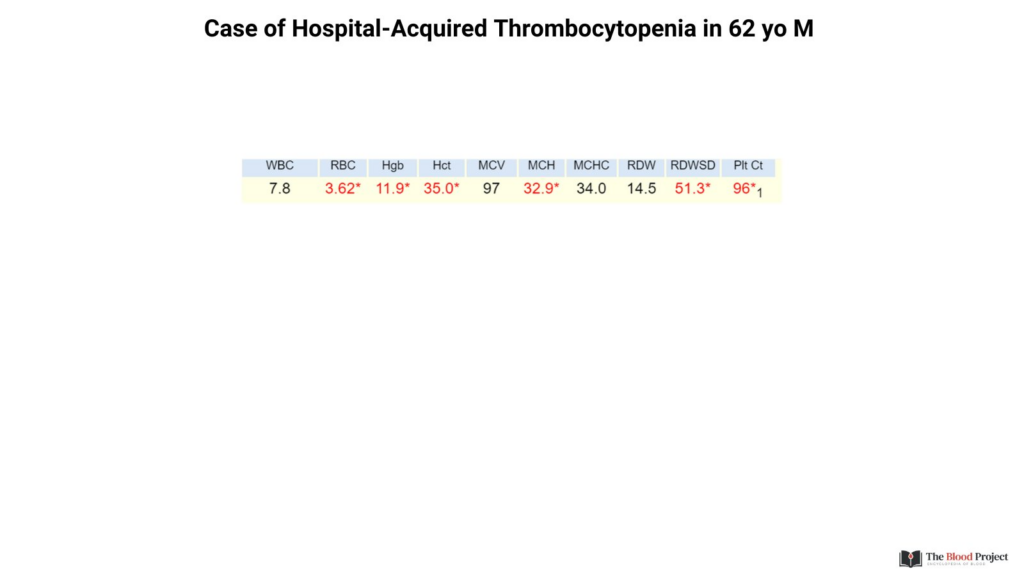
Check out the CBC in the graphic. This represents one time point during the hospital stay of a 62 yo man whose platelet count was normal on admission (that’s all the history you get).
When approaching the ddx of thrombocytopenia it is tempting to resort to the pathophysiological classification of decreased production, increased destruction/consumption and sequestration…
However, such an approach has poor discriminatory power since most conditions cause increased destruction/consumption of platelets. A more productive approach is to consider thrombocytopenia from the standpoint of the clinical context:
- Outpatient
- Inpatient
- Urgent care
Our patient developed thrombocytopenia as an inpatient. There are two MAJOR causes of hospital-acquired thrombocytopenia:
- Infection (with or without DIC)\
- Medication (heparin and non-heparin agents)
There are a number of LESS COMMON causes shown in the graphic:
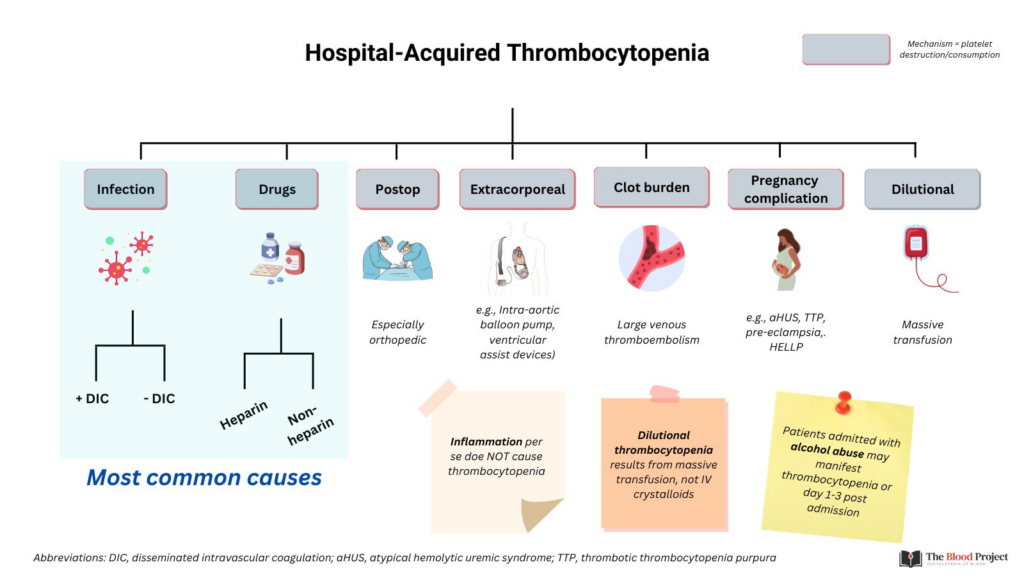
It is not uncommon for physicians-in-training to invoke “inflammation” as a cause of de novo thrombocytopenia in hospital. Inflammation may cause anemia, leukocytosis and thrombocytosis. It does not cause thrombocytopenia (an exception is HLH).
Another common error is to attribute inpatient thrombocytopenia to crystalloids (“dilutional”). CONSDER: If a patient with a Hb 13 and PLT 300 gains 20% blood volume with crystalloid, their Hb with fall to 10.4 (dilutional anemia), but PLTs remain in normal range (240).
Our patient was not taking heparin or other new medications implicated in thrombocytopenia (e.g., vancomycin, chemotherapy), did not have a clot, was not on an extracorporeal machine, was not postop and had not received massive transfusions.
What next test would you order?
- Maybe a peripheral smear? Red cell morphology was normal
- How about DIC screen? PT, PTT and fibrinogen were all normal
- Blood cultures? Pending
What are the chances the patient has a serious infection? You might point to the normal white cell count as evidence against such a diagnosis. Would you order a white cell differential?
Well, a differential was ordered and it showed a massive left shift:
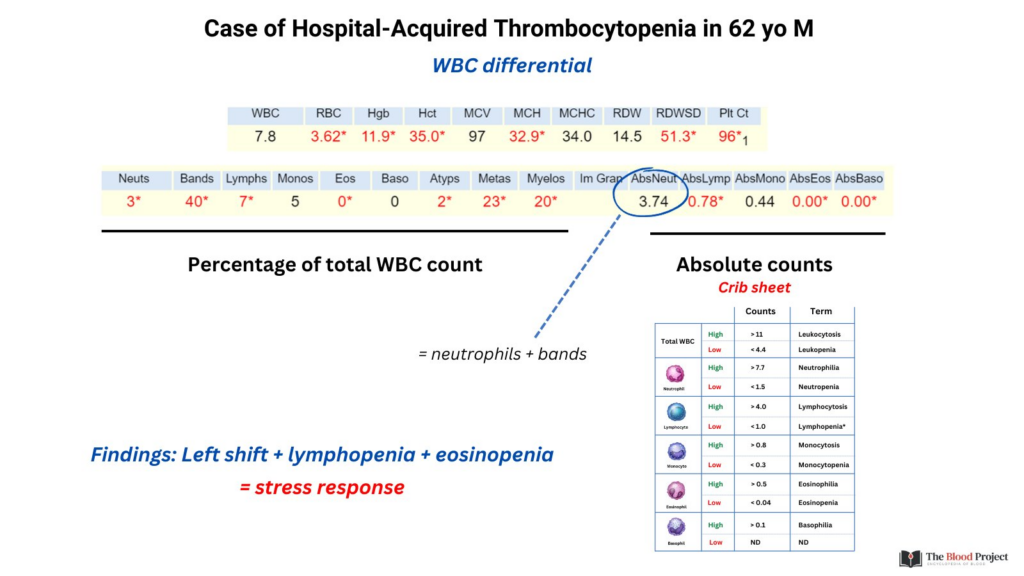
This is a nice example of how a normal WBC count may belie a n abnormal differential.
The patient had septic shock secondary to multifocal pneumonia and infection-associated thrombocytopenia.