Postscript
Introduction
- D-dimer is a plasmin-derived soluble degradation product of cross-linked fibrin.
- D-dimer can be measured in whole blood or in plasma.
- Healthy individuals have low but detectable levels of circulating D-dimer, resulting from near constant physiological conversion of fibrinogen to fibrin.
- There are many causes for an elevated D-dimer level; the D-dimer testing has:
- Poor specificity and positive predictive value for diagnosing venous thromboembolism (VTE).
- Limited clinical utility.
- D-dimers are most useful:
- In diagnostic algorithms to exclude a diagnosis of VTE in those with low clinical probability for this condition.
- To determine the optimal duration of anticoagulation in VTE patients.
- In the diagnostic algorithm for disseminated intravascular coagulation (DIC).
- The role of D-dimer in patients with other conditions such as predicting the risk of stroke in atrial fibrillation, identifying patients with coronary artery disease or human immunodeficiency virus (HIV) infection at risk for cardiovascular events, or for ruling out acute aortic dissection remains uncertain.

Generation of fibrinopeptides and fibrin monomers and polymer occurs after the action of thrombin on fibrinogen, prior to the formation of thrombi, while D-dimers and other fibrin degradation products are created by the action of plasmin on cross-linked fibrin. Fibrinogen degradation products are formed by the action of plasmin on fibrinogen.
Normal range
- Normal plasma levels of D-dimer by ELISA testing are <500 ng/mL for fibrin equivalent units (FEU) or <250 ng/mL for D-dimer units (DDU).
Causes of elevated D-dimers
- Individuals with suspected thrombosis:
- D-dimer levels are increased in almost all cases of acute thrombosis, including:
- Arterial:
- Myocardial infarction
- Stroke
- Acute limb ischemia
- Intracardiac thrombus
- Venous:
- Deep vein thrombosis
- Pulmonary embolism
- Disseminated intravascular coagulation (DIC)
- Arterial:
- D-dimer levels are increased in almost all cases of acute thrombosis, including:
- Individuals without evident thrombosis:
- D-dimer is not a specific test for venous thromboembolism (VTE). It may be elevated in patients who have other diagnoses, such as:
- Tissue injury:
- Minor and major trauma
- Surgery
- Interventional procedures
- Inflammation, including infection
- Liver disease
- Vascular disorders:
- Vascular malformations
- Sickle cell disease vaso-occlusion
- Acute aortic dissection (AAD)
- Aortic aneurysm
- Thrombolytic therapy
- Malignancy
- Pregnancy:
- Normal pregnancy
- Preeclampsia and eclampsia
- Anxiety
- Following exercise
- Elderly
- D-dimer levels increase with age.
- The upper 95th percentile for D-dimer is 2.5 times greater in people over the age of 70 compared to people less than 50 years old.
- Tissue injury:
- D-dimer is not a specific test for venous thromboembolism (VTE). It may be elevated in patients who have other diagnoses, such as:
- Cohort study of 581 hospitalized patients with D-dimer > 5,000 mcg/L:
- Pulmonary embolism (PE) 32%
- Cancer 29%
- Sepsis 24%
- Trauma 24%
- DVT 13%
- Cohort study in which D-dimer assay performed on 647 patients presenting to the emergency department with suspicion of VTE. Only patients with D-dimer values >243 ng/mL were included:
- Infection 15.6%
- VTE 12.1%
- Syncope 9.4%
- Heart failure 8.9%
- Trauma 8.2%
- Cancer 5.8%
- Cohort study in which D-dimer assay performed on 813 patients presenting to the emergency department:
- 148 emergency patients with D-dimer levels higher than 5.0 µg/mL. Diagnoses included:
- Sepsis 24.3%
- Malignancy 14.9%
- Trauma 13.5%
- VTE 11.5%
- CVA 11.5%
- Aortic dissection 6.8%
- cirrhosis 6.8%
- 148 emergency patients with D-dimer levels higher than 5.0 µg/mL. Diagnoses included:
Mechanisms
- Fibrinogen is a soluble plasma glycoprotein that is transformed into highly self-adhesive fibrin monomers after thrombin cleavage of fibrinopeptides A and B.
- This process is then followed by rapid polymerization of fibrin monomers, which is in turn followed by association of C-terminal extremities of gamma-chains catalyzed by activated factor XIII, a process which produces the dimerization of D-domains between nearby fibrin monomers.
- The subsequent lysis of “crosslinked” fibrin, mostly catalyzed by plasmin, generates a large array of products containing the fibrin fragments DD and E. The generation of dimeric D-domains (“D-dimers”) reliably reflects fibrin formation and dissolution.
- D-dimer levels indicate the balance between:
- The rate and magnitude of intravascular and extravascular fibrin formation.
- The clearance of D-dimers.
- Any process that increases fibrin production or breakdown also increases D-dimer levels.
- An elevated D-dimer level suggests persistent activation of clotting or inflammatory pathways.
| Cause of elevated D-dimer | Mechanism |
|---|---|
| VTE | Plasmin-mediated breakdown of clot-containing fibrin. |
| Tissue injury | Tissue injury is followed by clot formation, which then promotes wound healing. |
| Inflammation | Proteins leak into the extravascular space, where coagulation proteins escape the blood vessel and form an extravascular clot in the interstitial space. These clots are broken down similarly to intravascular clots, resulting in the formation of extravascular D-dimers, which are then absorbed into the blood and are readily detectable by blood tests. |
| Liver disease | D-dimers are cleared by the mononuclear phagocyte system in the liver and spleen. |
| Malignancy | Significant intravascular and extravascular fibrin formation (with extravascular fibrinolysis in the cancer stromal spaces) occurs in patients with cancer. |
| Exercise | Increased plasminogen activator levels. |
| Anxiety | Increased plasminogen activator levels. |
| Elderly | Furthermore, during the aging process, inflammation and activation of blood coagulation may also be enhanced and account for elevated baseline D-dimer levels seen in the elderly. |
Diagnosis
- D-dimer in whole blood or plasma is detected with monoclonal antibodies that recognize an epitope on cross-linked D-dimer that is absent in the D domain of fibrinogen and non–cross-linked fibrin monomers.
- The process of measuring D-dimer can be divided into two steps:
- D-dimer fragments must be captured by monoclonal antibodies.
- Captured antibodies are immobilized on a larger structure, such as a microplate well or membrane, or linked to a latex bead or red cell.
- D-dimer plus monoclonal antibodies must be detected and quantified.
- Detection antibodies can be labeled and produce a colorimetric or fluorescent reaction that is quantified after binding captured D-dimer or can be linked to a large particle such as a bead or red blood cell to induce agglutination.
- D-dimer fragments must be captured by monoclonal antibodies.
- Although there are numerous commercial D-dimer assays, they are of 3 general types:
- Whole-blood agglutination assays:
- Use a bispecific antibody conjugate that binds to D-dimer and a red blood cell membrane antigen such that red blood cell agglutination occurs when D-dimer levels are elevated.
- If D-dimer antigen is present, erythrocyte agglutination occurs.
- Whole blood agglutination assays are semiquantitative and yield positive or negative results.
- Plasma D-dimer levels:
- Enzyme-linked immunosorbent and enzyme-linked immunofluorescent assays (ELISA and ELFA, respectively):
- Rely on the use of 2 monoclonal antibodies—one that captures the D-dimer in the sample, and a second labeled antibody that is used to tag and quantify the captured D-dimer.
- Enzyme-linked immunosorbent assays (ELISA):
- For microplate ELISA, plasma is added to microtiter wells that are coated with D-dimer antibody. After incubation, a second labeled antibody also specific for D-dimer is added to the well that binds to immobilized D-dimer molecules and then produces a colorimetric reaction.
- Time consuming and require specialized personnel and therefore are impractical for routine D-dimer determination.
- Enzyme-linked immunofluorescence assays (ELFA):
- Designed along the same principles as the microplate ELISA, ELFAs are fully automated and binding of the detection antibody produces a fluorescent product.
- These assays have a rapid turnaround time and can be performed on single samples.
- Latex agglutination assays:
- Use immunoturbidometric techniques to detect D-dimer conjugated to antibody-coated latex
beads. Latex agglutination assays are popular because they can be performed using automated coagulation analyzers. - Available in qualitative, semiquantitative, and quantitative formats.
- Second-generation latex-enhanced immunoturbidimetric assays are fully automated, quantitative assays that measure transmission of light with a photometric analyzer.
- Second-generation latex-enhanced immunoturbidimetric assays are fully automated, quantitative assays that measure transmission of light with a photometric analyzer.
- Use immunoturbidometric techniques to detect D-dimer conjugated to antibody-coated latex
- In a meta-analysis of over 300 studies, ELISA, ELFA, and quantitative latex agglutination assays were more sensitive than whole-blood agglutination assays. Therefore, unless other assays are unavailable, the whole-blood D-dimer assay should not be used.
- Enzyme-linked immunosorbent and enzyme-linked immunofluorescent assays (ELISA and ELFA, respectively):
- Whole-blood agglutination assays:
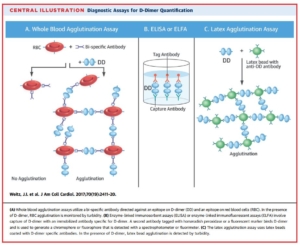
From J Am Coll Cardiol 2017;70:2411–20.
- D-dimer testing is further complicated by lack of a standardized unit of measure. D-dimer levels are reported as a unit of mass per volume. D-dimer levels are reported either as:
- D-dimer concentration in assays that use purified D-dimer as the calibrator (purified D-dimer units (DDUs))
- Fibrinogen equivalent units (FEUs) in those that use D-dimer–containing fragments that are generated
by clotting fibrinogen in the presence of factor XIIIa and then exposing it to limited plasmin digestion. Fibrinogen equivalent units can be converted to D-dimer concentration by dividing the level in half.- FEUs express the mass of D-dimer as the equivalent mass of fibrinogen that would be needed to
produce the D-dimer in the sample - One FEU has approximately two times the mass of one DDU; therefore, 1 μg/L of D-dimer as measured
in DDU is about equal to 2 μg/L in FEU.
- FEUs express the mass of D-dimer as the equivalent mass of fibrinogen that would be needed to
- Notes:
- Several assays and instruments are suited for either central laboratory or point-of-care testing:
- Central laboratory assays use either enzyme-linked immunosorbent assay (ELISA) technology or immunoturbidimetric assays.
- Point-of-care assays are read by visually inspecting the development of color on a slide and are designated as moderately sensitive.
- Central laboratory assays are more sensitive than point-of-care assays.
- Each manufacturer of D-dimer tests uses a specific monoclonal antibody and unique detection methodology to quantify D dimer in clinical samples.
- Threshold or cutoff level (“positive” and “negative” result) is determined by the manufacturer.
- Maximizing sensitivity comes at the cost of lowering specificity. If specificity is too low, the end result is reduced clinical utility of the assay because few patients will have a negative result (i.e. the majority will have a positive test and need to proceed to diagnostic imaging).
- Several assays and instruments are suited for either central laboratory or point-of-care testing:
Clinical uses of D-dimer assay
- The D-dimer test is a sensitive assay for any disease process that causes intravascular or extravascular injury through infection, inflammation, cancer, or trauma. Clinical uses, however, are largely limited to:
- Diagnosing venous thromboembolism (VTE).
- Determining duration of anticoagulation in VTE.
- Diagnosing disseminated intravascular coagulation (DIC).
- Venous thromboembolism:
- Diagnosis:
- D-dimers are detectable at levels above 500 ng/mL in virtually all patients with VTE.
- D-dimer testing is an integral part of validated algorithms for the diagnosis of deep-vein thrombosis (DVT) and pulmonary embolism (PE).
- Because of its good sensitivity for detection of thrombosis and its poor specificity, the D-dimer test is best used diagnostically to exclude VTE rather than to confirm it. D-dimer measurements combined with diagnostic imaging have a high negative predictive value in the diagnosis of DVT, and are used to limit the use of more expensive and invasive studies.
- The pretest probability of DVT is a major determinant of the potential value of D-dimer measurement.
- The D-dimer is most useful when the clinical pretest probability score for DVT or PE is low:
- Low clinical pretest probability score plus a low D-dimer value can rule out the need for further testing (with ultrasound) because DVT will develop in only 0.4 % of such patients.
- Diagnosis of VTE in outpatients usually starts with assessment of clinical pre-test probability using validated scoring systems such as the Wells score for DVT and the Wells or Geneva score for PE.
- Using such scores, clinical pre-test probability is categorized as likely or unlikely, or as high, intermediate, or low. The clinical pre-test probability is used to guide further testing.
- If VTE is unlikely, D-dimer testing is the next step.
- D-dimer testing is of limited value in patients with a high pre-test probability because even if the D-dimer level is normal, the negative predictive value of the test is reduced by the high prevalence of VTE in such patients.
- Therefore, if the pre-test probability is high, patients should go directly to diagnostic testing with compression ultrasonography for DVT and computed tomography pulmonary angiography for PE.
- Diagnosis:
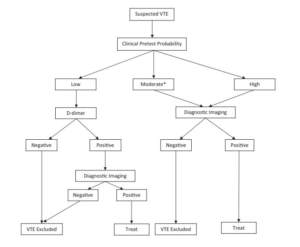
Diagnostic algorithm for venous thromboembolism. *D-dimer testing may also be performed to exclude VTE in this category depending on the assay used. From Int J Lab Hem. 2017;39(Suppl. 1):98–103.
-
-
- Caveats:
- D-dimer assay should not be used as stand-alone test to diagnose VTE.
- D-dimer levels vary with:
- Clot burden:
- Patients with large pulmonary emboli (PE) have higher D-dimer levels compared with those with smaller thromboses.
- Patients with deep vein thrombosis (DVT) that extends above the knee have higher D-dimer levels compared to patients who have thrombosis confined to their calf (proximal vs distal DVT).
- Time of measurement:
- Patients with confirmed DVT who have symptoms > 7 days in duration have lower D-dimer concentrations compared to patients with DVT and a shorter duration of symptoms.
- D-dimer levels fall quickly after initiation of anticoagulation. Within 24 hours of heparin treatment, D-levels fall by about 25%.
- Clot burden:
- The data above apply to patients without any history of active malignancy:
- The specificity of the D-dimer test in patients with cancer is reduced by the high prevalence of VTE and the higher rate of elevated D-dimer values in this patient population.
- Though studies have shown differing results, it appears that a negative D-dimer together with a low or unlikely pre-test probability excludes VTE in cancer patients like it does in those without cancer (though only about 15% of cancer patients meet these criteria).
- Therefore, most cancer patients with suspected VTE should undergo diagnostic imaging rather than D-dimer testing.
- The data above apply to outpatients.
- The D-dimer levels below the normal cutoff value that was used to exclude venous thrombosis was established in outpatients.
- The usefulness of D-dimer testing for the inpatient evaluation of VTE is limited.
- The diagnosis of thrombosis in this setting is complicated by the fact that D-dimer levels are often increased for various reasons in hospitalized patients (that do not necessarily result in overt thrombosis), which limits its value for exclusion of VTE.
- D-dimer testing for diagnosis of VTE should be avoided in situations where it is expected to be positive, such as after major surgery or trauma or in hospitalized medical patients, particularly those in the intensive care unit. Because of the high frequency of false-positive results in these settings, using D-dimer to screen for VTE increases the need for additional testing.
- Caveats:
- Determining duration of anticoagulation:
- The optimal duration of anticoagulant therapy in patients with a first unprovoked DVT or PE is unclear. Such patients require at least 3 months of anticoagulant therapy, and current guidelines suggest extending anticoagulation treatment, provided that the risk of bleeding is not high.
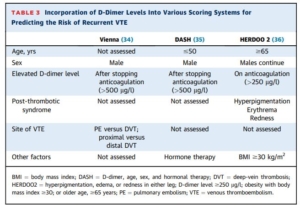
- In this subgroup of patients, patient sex and D-dimer level measured about 1 month after stopping anticoagulant therapy (posttreatment D-dimer) can help to further stratify the risk of recurrent VTE:
- The risk of recurrence is higher in:
- Men than women (1.75-fold relative risk).
- Those with elevated D-dimers (about 2-fold relative risk).
- Risk of recurrence in women:
- With a negative posttreatment D-dimer similar to that in patients with a proximal DVT or PE that was provoked by a minor transient risk factor (approximately 15% recurrence at 5 years).
- With a positive posttreatment D-dimer about 30%.
- Therefore, D-dimer testing in women may be helpful in deciding whether or not to continue anticoagulation (negative D-dimer, stop; positive D-dimer, continue).
- The risk of recurrence in men with a negative D-dimer is not much less than the overall risk of recurrence that we have estimated for patients with an unprovoked proximal DVT or PE (approximately 25% compared with approximately 30% recurrence at 5 years); consequently, the argument for extended anticoagulation in these men is still substantial, suggesting that D-dimer testing will often not influence a male’s decision.
- D-dimer levels have been incorporated into risk prediction models, including the HERDOO2 (hyperpigmentation, edema, or redness in either leg; D-dimer level >250 mg/l; obesity with body mass index >30; or older age, >65 years) rule and the DASH (D-dimer, age, sex, and hormonal therapy) and Vienna scores.
-
-
- Other examples where D-dimer testing may be helpful in the setting of VTE:
- COVID-19:
- COVID-19 has been associated with inflammation and a prothrombotic state, with increases in levels of fibrin, fibrin degradation products, fibrinogen, and D-dimer.
- Elevated D-dimers are believe to originate more from intense inflammation (resulting in extravascular fibrinolysis and thus production of large amounts of D-dimers) than intravascular thrombus formation.
- D-dimer levels are higher in patients with COVID-19, especially those with severe or critical disease, independent of the presence or absence of PE/VTE, and so their use for diagnosing VTE is limited (since the levels are high in most patients).
- The presence of high D-dimer levels have been shown to be associated with more severe COVID-19. Elevated levels have been used in some trials of anticoagulants to risk stratify patients. Whether elevated D-dimer level alone predicts response is unclear, with trials showing variable results.
- Low D-dimer levels are of high negative predictive value for excluding cerebral venous thrombosis in patients with isolated headache (BMC Neurol. 2015;15:118)
- Elevated D-dimer levels over twice the upper limit of normal identify medically ill patients at increased risk of VTE who may benefit from extended prophylaxis.
- COVID-19:
- Other examples where D-dimer testing may be helpful in the setting of VTE:
- Disseminated intravascular coagulation:
- No single laboratory test is specific for DIC.
- Initial abnormalities include:
- Decreased platelet count
- Elevated fibrin degradation products or D-dimer
- Elevated prothrombin time (PT) and activated partial thromboplastin time (aPTT)
- Reduced fibrinogen (more commonly observed during acute phase of DIC)
- Clinical prediction rules help identify patients with DIC using clinical information and results from a panel of blood tests. All diagnostic scoring systems include elevated fibrin-related marker (D-dimer or FDP).
What do the Guidelines say?
- American Society of Hematology 2018 guidelines for management of venous thromboembolism: diagnosis of venous thromboembolism:
- Diagnosis of pulmonary embolus:
- Low pretest probability (PTP)/prevalence (<5%):
- Recommendation 1a. The American Society of Hematology (ASH) guideline panel recommends using a strategy starting with D-dimer for excluding PE in a population with low prevalence/PTP (<5%), followed by ventilation-perfusion (VQ) scan or computed tomography pulmonary angiography (CTPA) for patients requiring additional testing. If D-dimer is not readily available,
alternate acceptable strategies include performing VQ scan or CTPA alone. (Strong recommendation for D-dimer based on high certainty in the evidence of effects on clinical outcomes).- For patients presenting to an emergency department with a low probability of PE, the Pulmonary Embolism Rule-out Criteria (PERC) may be used to determine whether D-dimer testing is warranted.
- If the D-dimer strategy is followed, a highly sensitive D-dimer assay is required.
- A negative D-dimer rules out PE and no additional testing or anticoagulation is required.
- D-dimer has limited utility in hospitalized patients and in certain patient populations (postsurgical, pregnant) due to the high frequency of positive D-dimer results with standard thresholds.
- Use of an age-adjusted D-dimer cutoff in outpatients older than 50 years is as safe as the standard cutoff and increases the diagnostic utility of the test. Age-adjusted cutoff 5 age (years) 3 10 mg/L (using D-dimer assays with a cutoff of 500 mg/L).
- Recommendation 1a. The American Society of Hematology (ASH) guideline panel recommends using a strategy starting with D-dimer for excluding PE in a population with low prevalence/PTP (<5%), followed by ventilation-perfusion (VQ) scan or computed tomography pulmonary angiography (CTPA) for patients requiring additional testing. If D-dimer is not readily available,
- Intermediate PTP/prevalence (∼20%).
- Recommendation 2a. The ASH guideline panel suggests using a strategy starting with D-dimer for excluding PE in a population with intermediate prevalence/PTP (;20%), followed by VQ scan or CTPA for patients requiring additional testing. If D-dimer is not readily available, alternate acceptable strategies include performing VQ scan or CTPA alone. Patients who are likely to have a nondiagnostic VQ scan should undergo CTPA. (Conditional recommendation for D-dimer based on
high certainty in the evidence of effects on clinical outcomes).- If the D-dimer strategy is followed, a highly sensitive D-dimer assay is required.
- A negative D-dimer rules out PE and no additional testing or anticoagulation is required.
- D-dimer has limited utility in hospitalized patients and in certain patient populations (postsurgical, pregnant) due to the high frequency of positive D-dimer results with standard thresholds.
- Recommendation 2a. The ASH guideline panel recommends against using a positive D-dimer alone to diagnose PE, and against additional testing following negative CTPA or normal VQ scan in a population with intermediate prevalence/PTP (;20%). (See grading for recommendation 2a.)
- Recommendation 2a. The ASH guideline panel suggests using a strategy starting with D-dimer for excluding PE in a population with intermediate prevalence/PTP (;20%), followed by VQ scan or CTPA for patients requiring additional testing. If D-dimer is not readily available, alternate acceptable strategies include performing VQ scan or CTPA alone. Patients who are likely to have a nondiagnostic VQ scan should undergo CTPA. (Conditional recommendation for D-dimer based on
- High PTP/prevalence (>50%).
- Recommendation 3a. The ASH guideline panel suggests using a strategy starting with CTPA for assessing patients suspected of having PE in a population with high prevalence/PTP (>50%). (Conditional recommendation for CTPA based on very low certainty in the evidence of effects on clinical outcomes).
- If CTPA is not feasible (eg, contrast dye allergy, renal impairment, unavailability), VQ scan may be acceptable if nondiagnostic scans are followed by additional testing.
- In cases where clinical suspicion for PE remains high with a negative initial CTPA, additional testing with VQ scan or proximal ultrasound of the lower extremities may be considered.
- Recommendation 3a. The ASH guideline panel suggests using a strategy starting with CTPA for assessing patients suspected of having PE in a population with high prevalence/PTP (>50%). (Conditional recommendation for CTPA based on very low certainty in the evidence of effects on clinical outcomes).
- Low pretest probability (PTP)/prevalence (<5%):
- Diagnosis of lower extremity DVT:
- Low PTP/prevalence (< or = 10%).
- Recommendation 5a. The ASH guideline panel recommends using a strategy starting with D-dimer for excluding DVT in a population with low prevalence/ PTP (#10%), followed by proximal lower extremity ultrasound or whole-leg ultrasound for patients requiring additional testing. If D-dimer is not readily available, alternate acceptable strategies include performing proximal lower extremity or whole-leg ultrasound alone. (Strong recommendation for D-dimer based on moderate certainty in the evidence of effects on clinical outcomes).
- If the D-dimer strategy is followed, a highly sensitive D-dimer assay is required.
- A negative D-dimer rules out DVT and no additional testing or anticoagulation is required.
- D-dimer has limited utility in hospitalized patients and in certain patient populations (postsurgical, pregnant) due to the high frequency of positive D-dimer results with standard thresholds.
- Recommendation 5b. The ASH guideline panel recommends against using a positive D-dimer alone to diagnose DVT, and against additional testing following negative proximal or whole-leg ultrasound in a population with low prevalence/PTP (#10%). (See grading for recommendation 5a.)
- Recommendation 5a. The ASH guideline panel recommends using a strategy starting with D-dimer for excluding DVT in a population with low prevalence/ PTP (#10%), followed by proximal lower extremity ultrasound or whole-leg ultrasound for patients requiring additional testing. If D-dimer is not readily available, alternate acceptable strategies include performing proximal lower extremity or whole-leg ultrasound alone. (Strong recommendation for D-dimer based on moderate certainty in the evidence of effects on clinical outcomes).
- Intermediate PTP/prevalence (∼25%).
- Recommendation 6a. The ASH guideline panel suggests using a strategy using whole-leg ultrasound, or starting with proximal lower extremity ultrasound for evaluating patients suspected of having DVT in a population with intermediate prevalence/PTP (∼25%). No further testing is required
if the whole-leg ultrasound is negative, but a negative initial proximal ultrasound should be followed by serial proximal ultrasound if no alternative diagnosis is identified. In an intermediate PTP population where the prevalence is lower, other potentially acceptable strategies include proximal lower extremity ultrasound alone with no additional follow-up testing for negative results, or a strategy starting with D-dimer for excluding DVT followed by proximal lower extremity ultrasound or whole-leg ultrasound for patients requiring additional testing.- Studies where patients are determined to have an intermediate PTP for DVT have prevalence estimates of ∼13% to 24%. A decision to use a D-dimer strategy in an intermediate PTP population assumes the prevalence is ∼15% or less. A decision to start with D-dimer assumes the results will be obtained in a timely manner and that the cost of D-dimer screening is offset
by avoiding unnecessary ultrasound for patients at intermediate PTP for DVT. - If the D-dimer strategy is followed, a highly sensitive D-dimer assay is required.
- A negative D-dimer rules out DVT and no additional testing or anticoagulation is required.
- D-dimer has limited utility in hospitalized patients and in certain patient populations (postsurgical, pregnant) due to the high frequency of positive D-dimer results with standard thresholds.
- Studies where patients are determined to have an intermediate PTP for DVT have prevalence estimates of ∼13% to 24%. A decision to use a D-dimer strategy in an intermediate PTP population assumes the prevalence is ∼15% or less. A decision to start with D-dimer assumes the results will be obtained in a timely manner and that the cost of D-dimer screening is offset
- Recommendation 6a. The ASH guideline panel suggests using a strategy using whole-leg ultrasound, or starting with proximal lower extremity ultrasound for evaluating patients suspected of having DVT in a population with intermediate prevalence/PTP (∼25%). No further testing is required
- Low PTP/prevalence (< or = 10%).
- Diagnosis of pulmonary embolus:
- American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism:
- Secondary prevention: continuation of anticoagulation after primary treatment:
- For patients with unprovoked DVT and/or PE, the ASH guideline panel suggests against routine use of prognostic scores, D-dimer testing, or ultrasound to detect residual vein thrombosis to guide the duration of anticoagulation:
- Indefinite anticoagulation is probably appropriate for the majority of patients with unprovoked VTE. However, in certain circumstances, such as when patients are undecided or the
balance between risks and benefits is uncertain, clinicians and patients may use prognostic scores, D-dimer testing, or ultrasound assessment for residual thrombosis from an initial DVT to aid in reaching a final decision. - “We judged the certainty in the evidence as low for the use of ultrasonography and as very low for the use of D-dimer and prognostics scores.”
- Indefinite anticoagulation is probably appropriate for the majority of patients with unprovoked VTE. However, in certain circumstances, such as when patients are undecided or the
- For patients with unprovoked DVT and/or PE, the ASH guideline panel suggests against routine use of prognostic scores, D-dimer testing, or ultrasound to detect residual vein thrombosis to guide the duration of anticoagulation:
- Secondary prevention: continuation of anticoagulation after primary treatment:
- ASH guideline on venous thromboembolism in the context of pregnancy:
- The panel identified the following additional research need: the role of D-dimer testing and clinical prediction rules in limiting the need for radiologic tests in pregnant women with suspected pulmonary embolism needs to be evaluated in well-designed management studies.
- The role of D-dimer testing and clinical prediction rules in the management of pregnant women with suspected DVT needs to be evaluated in well-designed management studies
- Antithrombotic Therapy for VTE Disease Second Update of the CHEST Guideline and Expert Panel Report:
- Whether and how to prescribe anticoagulants to patients with isolated distal DVT:
- Positive D-dimer (particularly when markedly so without an alternative reason) is a factor that may favor choosing anticoagulation.
- Whether to treat isolated subsegmental pulmonary embolism:
- In patients whose imaging and clinical features suggest a true-positive finding of isolated subsegmental pulmonary embolism (ISSPE), an elevated D-dimer level (particularly if the increase is marked and otherwise unexplained) may favor anticoagulation.
- Whether and how to prescribe anticoagulants to patients with isolated distal DVT:
- American College of Chest Physicians (ACCP) guideline and expert panel report on antithrombotic therapy for venous thromboembolism (VTE) disease (2016 update):
- In patients with a first VTE that is an unprovoked proximal DVT of the leg or PE and who have a (i) low or moderate bleeding risk (see text), we suggest extended anticoagulant therapy (no scheduled stop date) over 3 months of therapy (Grade 2B), and (ii) high bleeding risk (see text), we recommend 3 months of anticoagulant therapy over extended therapy (no scheduled stop date) (Grade 1B).
- Remarks: Patient sex and D-dimer level measured a month after stopping anticoagulant therapy may influence the decision to stop or extend anticoagulant therapy. In all patients who receive extended
anticoagulant therapy, the continuing use of treatment should be reassessed at periodic intervals (eg, annually) - The most common and difficult decision about whether to stop anticoagulants after a time-limited course or to use extended therapy is in patients with a first unprovoked proximal DVT or PE without a high risk of bleeding. In this subgroup of patients, patient sex and D-dimer level measured about 1 month after stopping anticoagulant therapy can help to further stratify the risk of recurrent VTE:
- Men have about a 75% higher (1.75-fold) risk of recurrence compared with women, whereas patients with a positive D-dimer result have about double the risk of recurrence compared with those with a negative D-dimer, and the predictive value of these two factors appears to be additive.
- The risk of recurrence in women with a negative posttreatment D-dimer appears to be similar to the risk that we have estimated for patients with a proximal DVT or PE that was provoked by a minor transient risk factor (approximately 15% recurrence at 5 years); consequently, the argument for extended anticoagulation in these women is not strong, suggesting that D-dimer testing will often influence a woman’s decision.
- The risk of recurrence in men with a negative D-dimer is not much less than the overall risk of recurrence that we have estimated for patients with an unprovoked proximal DVT or PE (approximately 25% compared with approximately 30% recurrence at 5 years); consequently, the argument for extended anticoagulation in these men is still substantial, suggesting that D-dimer testing will often not influence a male’s decision. Because there is still uncertainty about how to use D-dimer testing and a patient’s sex to make decisions about extended therapy in patients with a first unprovoked VTE, we have not made recommendations based on these factors.
- Remarks: Patient sex and D-dimer level measured a month after stopping anticoagulant therapy may influence the decision to stop or extend anticoagulant therapy. In all patients who receive extended
- In patients with a first VTE that is an unprovoked proximal DVT of the leg or PE and who have a (i) low or moderate bleeding risk (see text), we suggest extended anticoagulant therapy (no scheduled stop date) over 3 months of therapy (Grade 2B), and (ii) high bleeding risk (see text), we recommend 3 months of anticoagulant therapy over extended therapy (no scheduled stop date) (Grade 1B).