Treatment

Overview of treatment of thrombotic thrombocytopenic purpura (TTP):
Pathophysiological basis for treatment:
- von Willebrand factor (vWF) normally promotes interactions between platelets and the blood vessel wall.
- vWF circulates as multimers of varying size; the largest of these multimers (called ultra-large multimers) are the most functionally (hemostatically) active.
- Normally, the protease ADAMTS13, which is synthesized by the liver, cleaves circulating ultra-large vWF multimers, preventing excessive platelet-vessel wall interactions.
- Immune TTP is caused by antibody-mediated reduction in ADAMTS13 levels.
- ADAMTS13 deficiency results in excessive ultra-large vWF multimers, leading to uncontrolled platelet activation, adhesion and aggregation, microvascular thrombosis and tissue ischemia.
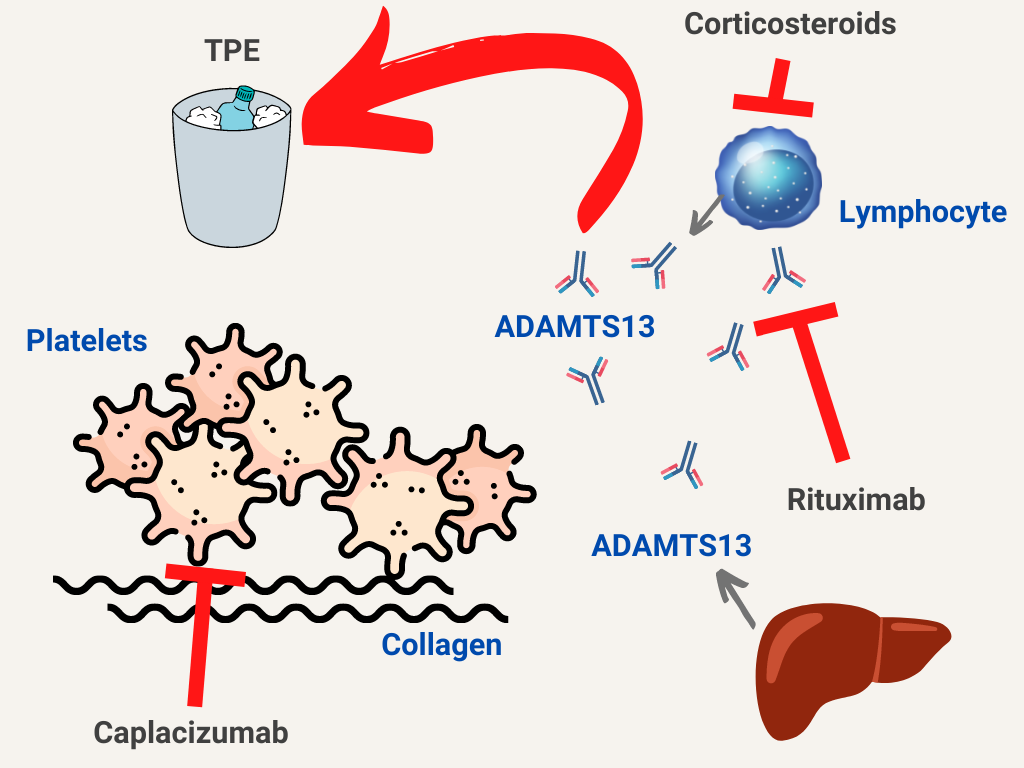
Treatment approaches:
- Remove antibodies against ADAMTS13 – therapeutic plasma exchange (TPE) – the mainstay of treatment
- Replenish ADAMTS13 – TPE
- Block von Willebrand factor-platelet interactions – caplacizumab
- Inhibit production of antibodies against ADAMTS 13 – corticosteroids, rituximab
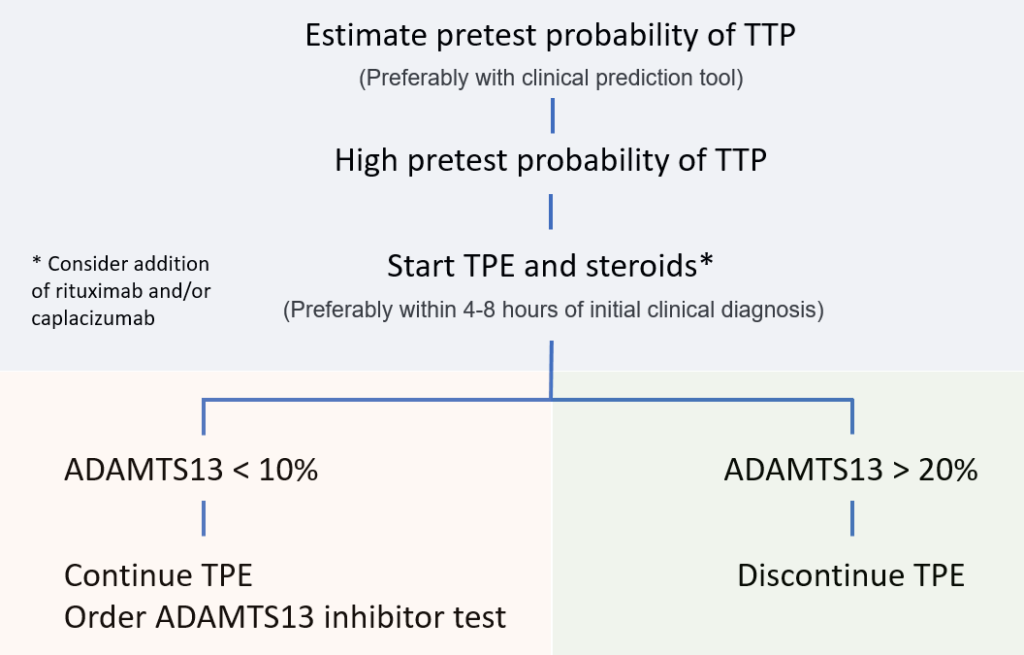
Overview of treatment pre- and post-ADAMTS13 levels: