Hyperferritinemia
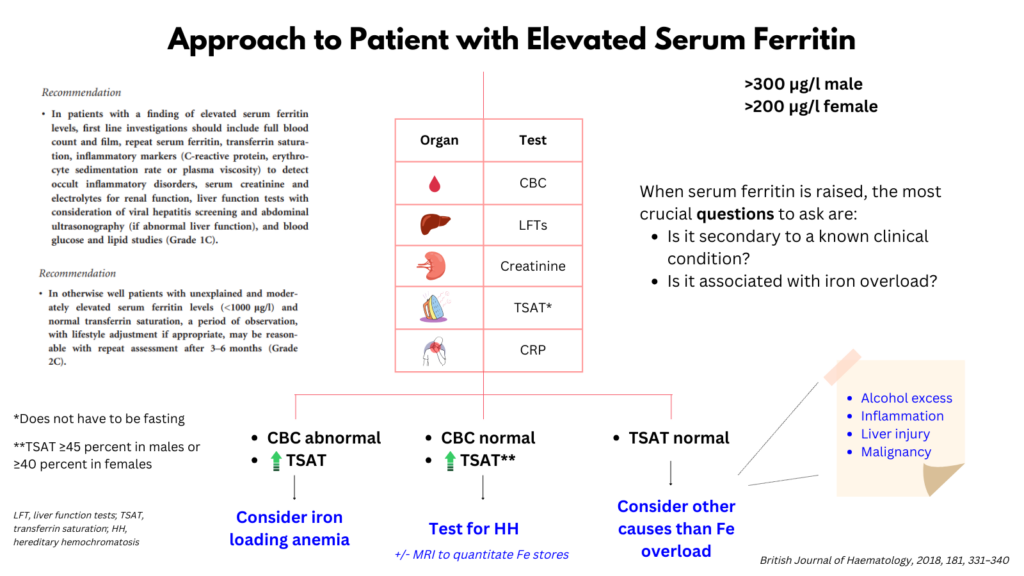
When approaching a patient with an elevated serum ferritin level, questions to consider are: 1) What is the mechanism of the elevation, and 2) what is the cause of the elevation?
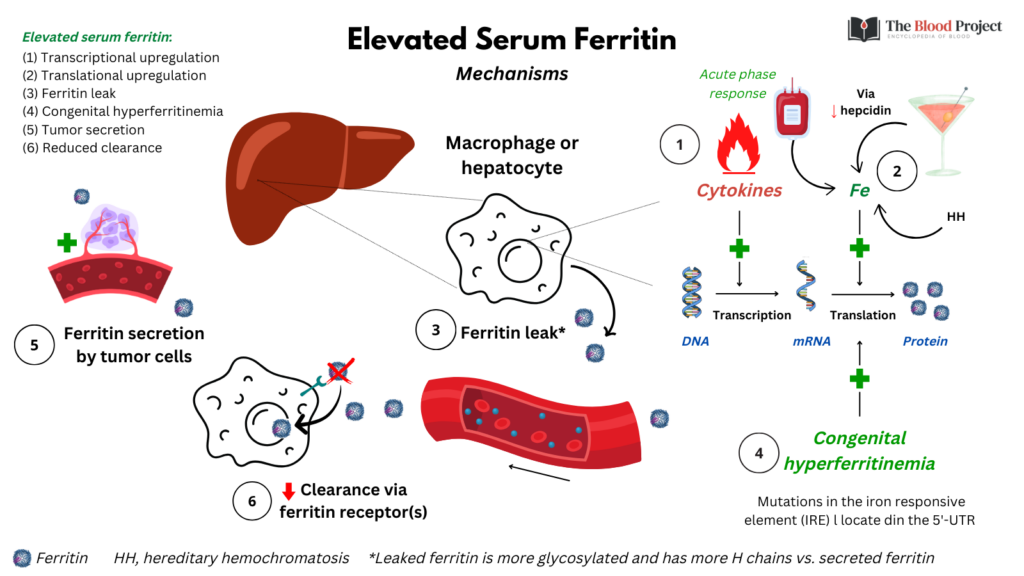
Mechanisms of hyperferritinemia
- Increased secretion of ferritin from macrophages, owing to increased ferritin levels from:
- Transcriptional upregulation, typically caused by elevated cytokine levels, including interleukin (IL)1, IL6, IL18, tumor necrosis factor-alpha, gamma-interferon and macrophage-colony stimulating factor.1
- Translational upregulation:
- Typically mediated by increased intracellular iron stores which leads to dissociation of iron regulatory proteins (IRF) from the iron-responsive element (IRE) in the 5′ untranslated region of FTH and FTL.
- May also be mediated by certain cytokines.
- Rarely caused by hereditary hyperferritinaemia-cataract syndrome.
- Ferritin leak, for example from:
- Hepatocytes in acute liver injuries such as alcoholic hepatitis.
- Macrophages in hemophagocytic lymphohistiocytosis2
- Secretion by tumor cells, for example glioblastoma cells34
- Reduced clearance (theoretically might increase ferritin levels)
Causes of elevated ferritin levels
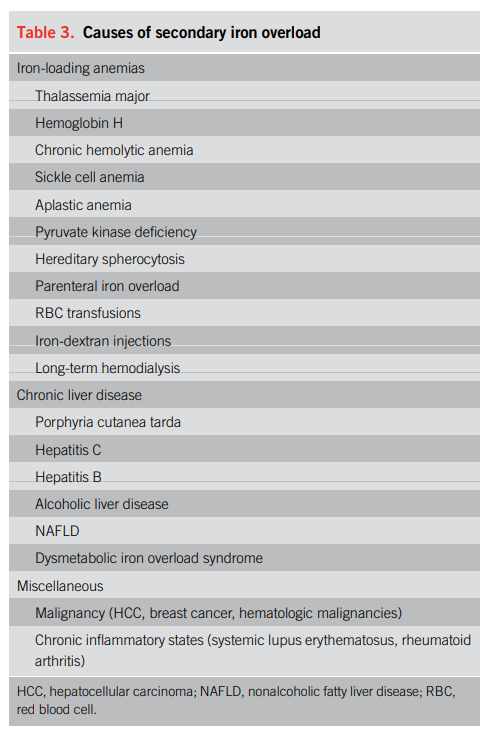
- Iron overload:
- Hereditary hemochromatosis:
- Most commonly caused by homozygous C282Y mutation on the HFE gene.
- Other gene mutations include those in the:
- HJV gene (hemojuvelin )
- HAMP gene (hepcidin)
- TFR2 gene (transferrin receptor-2)
- SLC40A1 gene (ferroportin disease)
- FTH1 gene (mutation in the iron responsive element of H-ferritin (FTH1) mRNA)
- Transfusional iron overload:
- Transfusional iron overload typically affects patients with hematologic disorders who require chronic red blood cell (RBC) transfusions, such as:
- Transfusion-dependent thalassemia
- Sickle cell disease
- Myelodysplastic syndrome (MDS)
- Transfusional iron overload typically affects patients with hematologic disorders who require chronic red blood cell (RBC) transfusions, such as:
- Ineffective erythropoiesis:
- Expanded erythroid marrow of patients with ineffective erythropoiesis results in erythroblast-mediated release of erythroferrone which inhibits the synthesis of hepcidin in the liver, resulting in increased iron absorption in the gut.
- Erythroid overproduction of erythroferrone causes iron overload in mice.5
- “In β-thalassemia, the release of increased amounts of erythroferrone by the expanded erythroid marrow suppresses hepcidin secretion, thus increasing iron absorption from the gut and iron release by reticuloendothelial cells and leading, in turn, to parenchymal iron overload, even in the absence of RBC transfusion”.6
- Alcohol:7
- Chronic alcohol consumers and those with alcoholic liver disease have been reported to demonstrate increased intestinal iron absorption (by twofold), serum ferritin, iron saturation of transferrin, and hepatic iron stores.
- Affected more by beer than wine or spirit consumption.8
- Alcohol reduces hepcidin synthesis in the liver, which:
- Results in reduced circulatory hepcidin levels
- Leading to increases serum iron levels
- Hereditary hemochromatosis:
- Inflammation:
- Ferritin is an acute phase protein that can be increased in the process of inflammation.
- Conditions include:
- Liver disease:
- Elevated serum ferritin is seen in almost any cause of liver injury.11
- Disturbances in iron homeostasis in liver diseases may be a manifestation of:
- Active inflammation
- Increase in liver iron
- Parenchymal damage with increased iron release from damaged/dead hepatocytes
- Acute:
- Acute hepatitis:
- Serum ferritin concentrations correlated with serum alanine transferase activity, especially in those with viral hepatitis. Believed to reflect the degree of macrophage activation in the liver.12
- Acute hepatic failure:
- Serum ferritin levels were significantly higher in fulminant hepatic failure and severe hepatitis than in acute hepatitis.13
- Acute hepatitis:
- Chronic:
- Serum ferritin levels are increased in patients with:14
- Chronic hepatitis B
- Chronic hepatitis C
- Chronic alcoholic liver disease
- Nonalcoholic fatty liver disease
- Autoimmune hepatitis
- Elevated serum ferritin levels reported to be independently associated with advanced liver fibrosis in patients with:15
- Chronic hepatitis C
- Nonalcoholic fatty liver disease
- Treatment-naive autoimmune hepatitis
- Serum ferritin levels paralleled serum aminotransferase levels in patients with AIH and chronic hepatitis C.16
- In patients with decompensated cirrhosis serum ferritin levels correlated with the severity of hepatic decompensation and were associated with a higher 15-day and 30- day mortality independent of the MELD score.17
- Serum ferritin levels are increased in patients with:14
- Hyperferritinemia-cataract syndrome (HHCS):18
- Automosomal dominant condition first described in 1995 and characterized by:
- High serum ferritin levels
- Congenital bilateral cataracts
- Absence of tissue iron overload
- Prevalence of the disease is 1 in 200,000 individuals
- Caused by mutations in the iron responsive element (IRE) located in the 5′ UTR of the Ferritin L mRNA (FTL).
- At least 47 causative mutations have been described in the FTL gene.
- IRE mutations lead to uncontrolled production of ferritin light chains (impervious to IRF-mediated inhibition of translation), resulting in elevated serum ferritin levels.
- Patients also present with bilateral cataracts at an early age are due to the accumulation of large amounts of crystal deposits formed by aggregated and iron-poor L-ferritin.
- Automosomal dominant condition first described in 1995 and characterized by:
Cohorts of patients with elevated serum ferritin levels
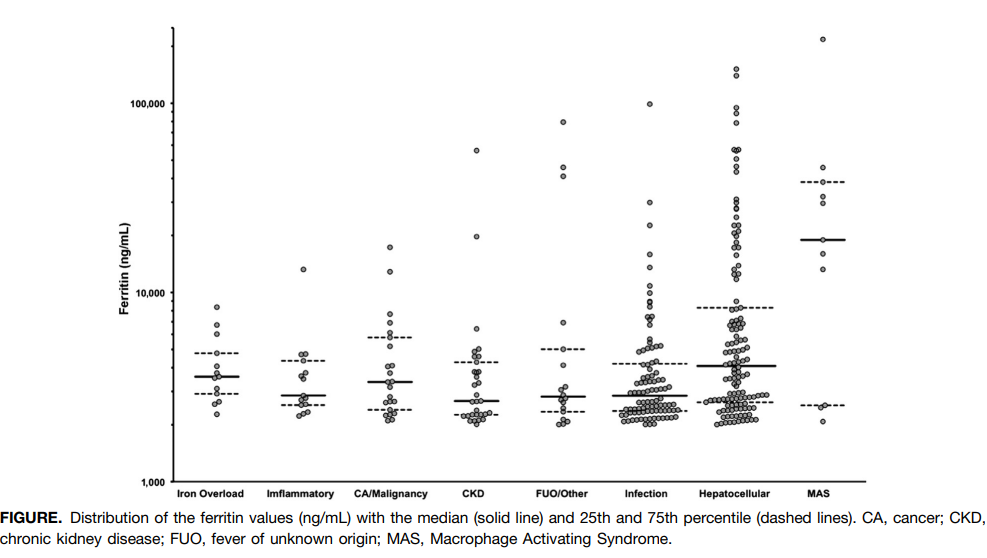
- Retrospective study of 333 adult inpatients with serum ferritin levels greater than 2,000 ng/mL:
- Hepatocellular injury was the most prevalent diagnosis with n = 126; infection was next with n = 96. Eleven patients were diagnosed with HLH/MAS.
- Authors conclude: “Elevated ferritin, as an isolated finding, was not a specific marker for the diagnosis of HLH/MAS. However, as a group, HLH/MAS patients had the highest mean and median ferritin values”.

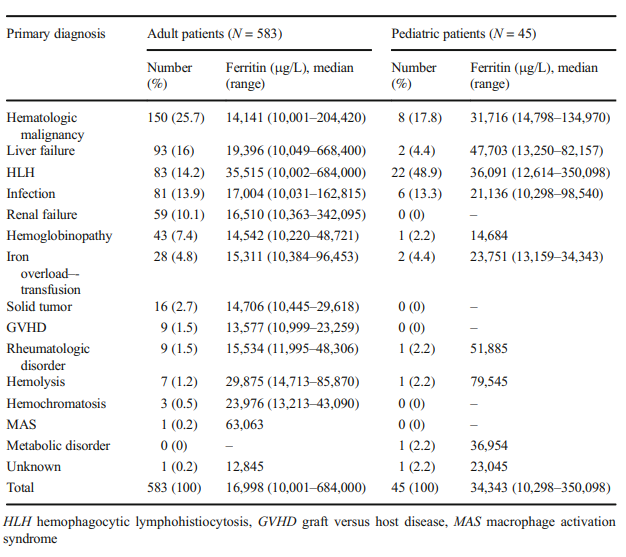
- Retrospective study of 196 pediatric and 583 adults and 45 pediatric patients with ferritin > 10,000 μg/L:
- The most common condition associated with elevated ferritin was hematologic malignancy in adults (25.7%) and HLH in pediatric patients (48.9%).
- HLH was diagnosed in 14.2% of adults and 48.9% of children with ferritin >10,000 µg/L.
- Authors concluded that: “Hyperferritinemia occurs in a variety of conditions and is not specific for adult or pediatric HLH. Common causes of elevated ferritin should be considered before entertaining the possibility of HLH, especially in adult patients”.

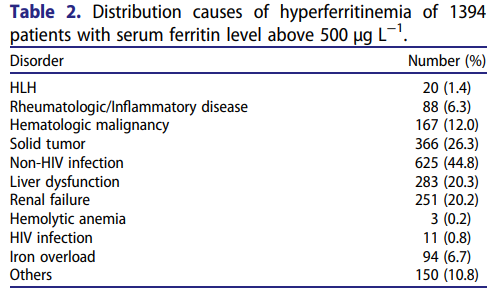
- Retrospective study of 1394 patients in Japan with ferritin measurement above 500 ng/ml:
- The most frequent causes of hyperferritinemia were:
- Non-human immunodeficiency virus infection
- Solid tumor
- Liver dysfunction
- Renal failure
- Hematological malignancy
- 40% had multiple causes
- The most frequent causes of hyperferritinemia were:
- Retrospective study of 2583 patients admitted to adult intensive care unit in Germany with hyperferritinemia of ≥500 ng//ml (Patients with HLH were excluded):
- Positive associations of maximum ferritin found with:
- Maximum SOFA score
- Sepsis or septic shock
- Liver disease (except hepatitis)
- Hematological malignancy
- Positive associations of maximum ferritin found with:
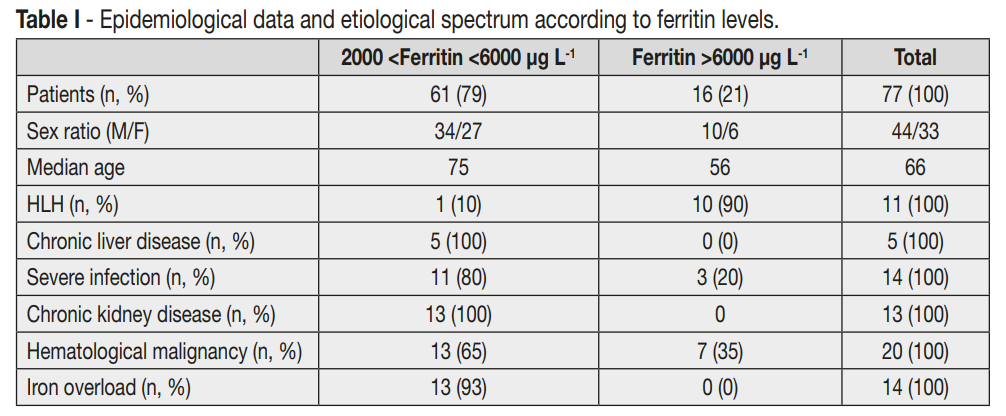
- Retrospective study of 77 patients in France with ferritin levels above 2000 ng/ml:
- Causes included
- Hematological malignancy (n=20)
- Severe infection (n=14)
- HLH (n=11)
- Causes included
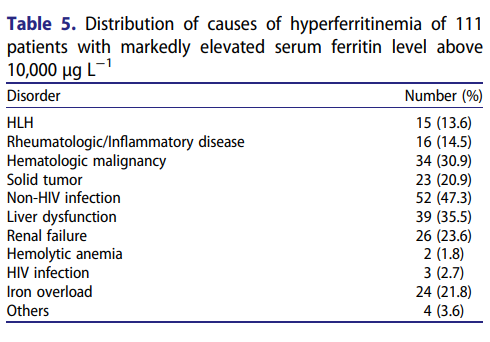
- Retrospective study of 113 patients with ferritin levels higher than 50,000 ng/ml:
- The most frequently observed conditions included:
- Renal failure
- Hepatocellular injury
- Infections
- Hematologic malignancies
- The authors conclude: “Highly elevated ferritin is not specific for hemophagocytic lymphohistiocytosis in adults.”
- The most frequently observed conditions included:

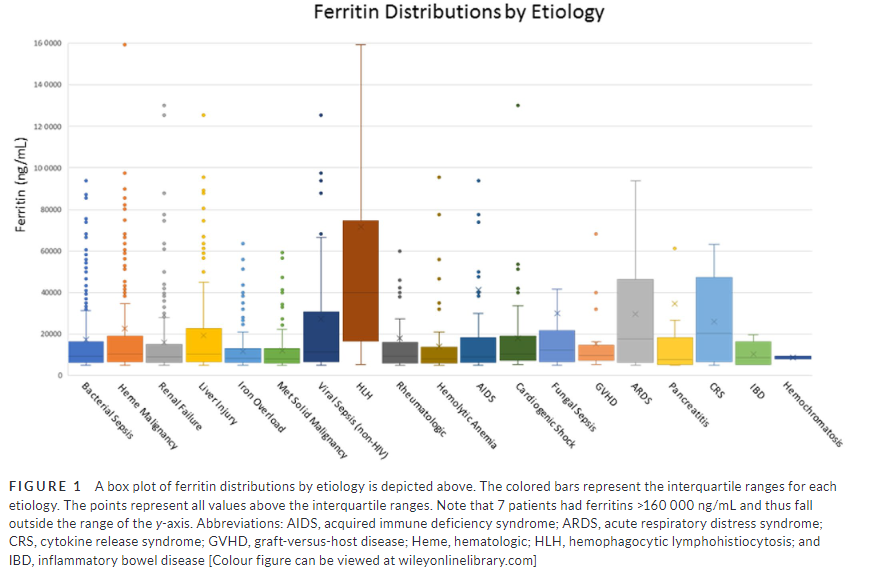
- Retrospective study of 1055 patients with serum ferritin >5000 ng/mL:
- HLH (6.5%)
- Mean ferritin among HLH patients was 70,398 ng/mL.
- The prevalence of HLH only reached 50% as serum ferritin approached 90,000 ng/mL.
- The optimal cutoff ferritin for diagnosis of HLH was 16 000 ng/mL (sensitivity 79.4%, specificity 79.2%, PPV 20.9%, and NPV 98.2%).
- Bacterial sepsis (33%)
- Hematologic malignancy (29%)
- Renal failure (24%)
- Liver injury (18%)
- HLH (6.5%)
Work up of patient with elevated serum ferritin